One of the most striking observations in global dementia epidemiology is a geographic and cultural disparity that has puzzled researchers for decades: the prevalence of Alzheimer's disease in rural India is among the lowest reported anywhere in the world.
The Cross-National Study
In the late 1990s, a collaboration between US and Indian researchers conducted the Indo-US Cross-National Dementia Epidemiology Study — a direct comparison of dementia rates in two populations using identical diagnostic criteria, assessment tools, and trained clinical teams.
The Indian arm examined residents of Ballabgarh, a town in Haryana, northern India. The US arm examined a comparable population in the Monongahela Valley of Pennsylvania.
| Population | Alzheimer's prevalence (age 65+) |
|---|---|
| Ballabgarh, India | ~1.07% |
| Monongahela Valley, Pennsylvania | ~4.4% |
A roughly 4-fold difference in Alzheimer's prevalence, measured with identical methodology.
Primary citation (prevalence data): Chandra V, Ganguli M, Pandav R, Johnston J, Belle S, DeKosky ST. (1998). Prevalence of Alzheimer's disease and other dementias in rural India: the Indo-US study. Neurology, 51(4):1000–1008.
PMID: 9781520
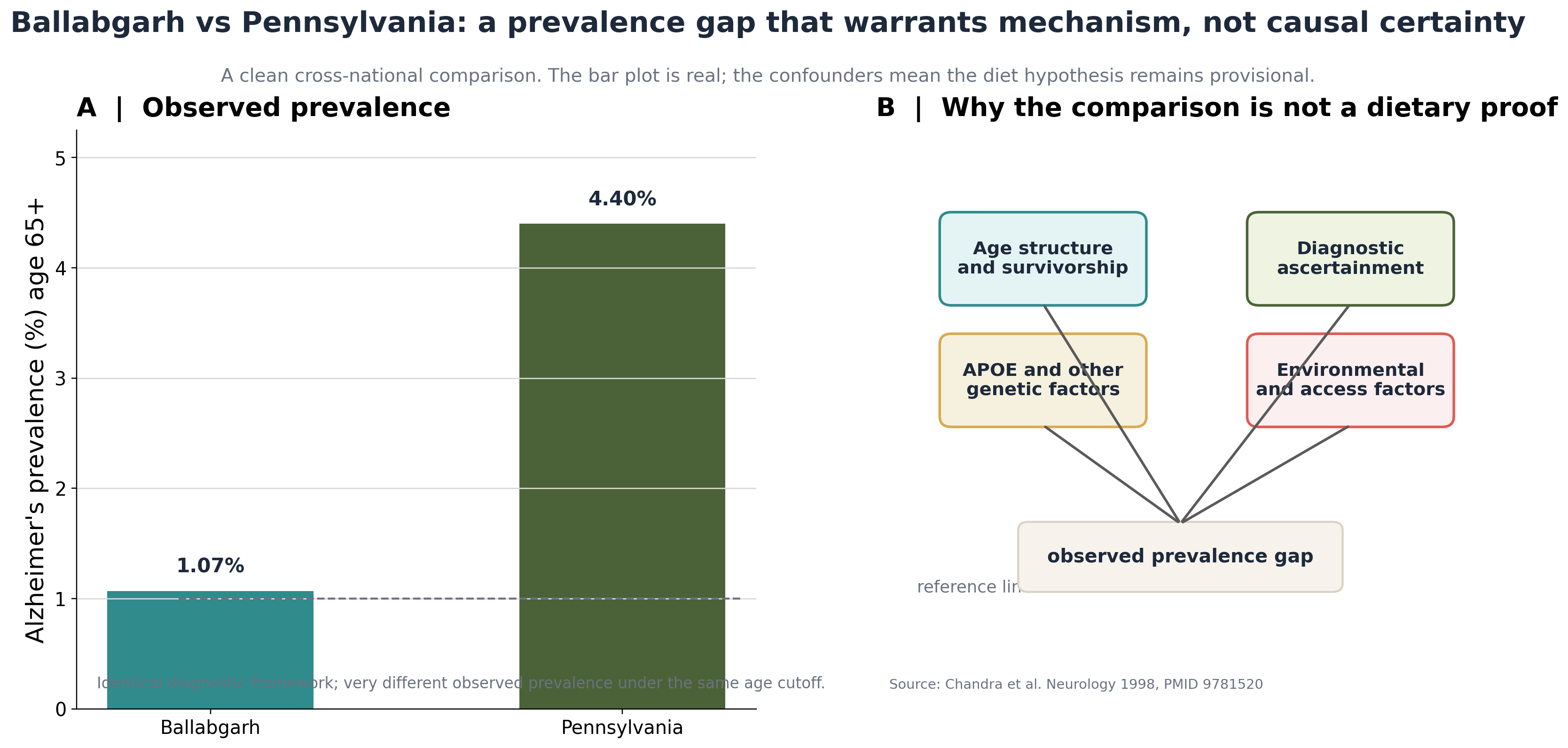
The prevalence gap is real, but so are the confounders. The comparison is strong enough to motivate a mechanism, not strong enough to prove one.
Observational comparison with explicit bias pathways shown on the right.
Why This Is Not Proof of a Dietary Effect
This is an observational prevalence comparison between two populations. Multiple factors beyond diet could explain the difference:
- Age structure: Populations with shorter life expectancy have fewer very elderly people at peak Alzheimer's risk. India's age pyramid in the 1990s was substantially younger than Pennsylvania's.
- Diagnostic ascertainment: Community-based detection rates vary with healthcare access, education levels, and the degree to which families seek diagnosis. Mild cognitive impairment is easily missed in settings without routine screening.
- Genetic background: The apolipoprotein E (APOE) ε4 allele — the strongest common genetic risk factor for late-onset Alzheimer's — has different frequency distributions across ethnic populations.
- Survivorship: Individuals who would have lived long enough to develop Alzheimer's in a high-mortality environment may not reach the age of onset.
The original researchers were explicit about these limitations. The finding is hypothesis-generating, not confirmatory of any specific dietary mechanism.
The Turmeric Hypothesis
The Ballabgarh–Pennsylvania disparity became prominent at a time when curcumin — the primary bioactive in turmeric — was being studied for its effects on amyloid-beta, the protein that aggregates into plaques in Alzheimer's disease.
Per-capita curcumin consumption in India through dietary turmeric has been estimated at approximately 100–500 mg per day — compared to near zero in typical Western diets. This contrast prompted the hypothesis that lifelong low-dose curcumin exposure might be neuroprotective.
Laboratory evidence in support of this hypothesis includes:
- Curcumin inhibits amyloid-beta aggregation in vitro
- It binds to existing amyloid fibrils and alters their structure
- It reduces neuroinflammation via NF-κB inhibition
- Animal studies show reduced amyloid plaque burden with curcumin supplementation
- Curcumin crosses the blood-brain barrier in sufficient quantities to reach brain tissue (established in animal studies; human brain pharmacokinetics are less well characterised)
What Clinical Trials Show
Despite extensive laboratory evidence and the epidemiological correlation, clinical trials of curcumin supplementation in Alzheimer's disease have not shown consistent benefit in patients with established disease. The hypothesis remains plausible for prevention — particularly at the population level over many decades of exposure — but has not been established by human intervention trials.
The gap between laboratory findings, population correlations, and clinical trial results is a recurring challenge in nutritional neuroscience. Several factors may contribute:
- Bioavailability: standard curcumin is poorly absorbed; enhanced formulations (with piperine, phospholipids, or nanoparticles) may be needed to achieve meaningful brain concentrations
- Timing: prevention trials would need to begin decades before symptoms appear — a study design challenge that applies to most preventive nutrition interventions
- Dose: dietary exposure and supplemental doses used in trials differ substantially
What This Finding Means for Research
The Ballabgarh–Pennsylvania comparison is one of the most compelling "natural experiments" in nutritional epidemiology. It illustrates the scientific value of cross-cultural prevalence comparisons: they can surface hypotheses that would be difficult to generate from within a single cultural or dietary context.
The correct interpretation is: the data motivates mechanistic investigation, not dietary prescription. It is a research signal, not a clinical recommendation.
No causal relationship between dietary turmeric and Alzheimer's prevention has been established in human clinical trials. The prevalence comparison is observational and multi-factorial. This content is for scientific information only and does not constitute medical advice or dietary recommendation.
Need a structured report on curcumin, clinical trial evidence, or cognitive nutrition for your audience?
Request a Report